CXL has shown promise in treating keratoconus and stabilizing corneal ectasia.
BY PETER S. HERSH, MD
RC, a 52-year-old man, presented with a history of corneal ectasia in his left eye, status post LASIK eight years earlier. Visual acuity in the unaffected right eye was 20/30 uncorrected and improved to 20/20 with -1.00 D sphere. Visual acuity in the left eye, however was 20/200 uncorrected and was best corrected to 20/80 with -2.50 -5.00 x 105. The patient complained of diplopia in his left eye. Corneal topography showed a maximum keratometry reading of 60.60 D.
Three decades ago, when I was new to treating keratoconus and other corneal ectatic disorders, this patient’s choices would have been limited to correction with glasses or gas permeable contact lenses, and a corneal transplant may have been inevitable. Since that time, however, researchers have learned not only how to manage the visual symptoms of keratoconus and post-LASIK ectasia, but to arrest the progress of the disease through corneal collagen crosslinking, or CXL.
Although not FDA approved, clinical studies under way or recently completed offer insight into the effectiveness of CXL, who is an ideal candidate and ways to improve the procedure, some of which I will look at here.
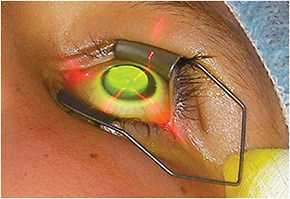
Patient undergoing accelerated crosslinking using the Avedro CXL system.
WHAT CXL CAN ACCOMPLISH
Corneal stiffness
In 1997, Theodore Seiler, MD, PhD, and his team at the University of Dresden in Germany began investigating whether inducing cross-links in corneal tissue would increase corneal stiffness, possibly leading to a future treatment for keratectasia.1,2 They found that treatment with riboflavin and UV-irradiation resulted in increased corneal stiffness.
Crosslinking takes advantage of two processes. First, ultraviolet radiation itself will tend to form crosslinks within collagen through a photobiologic process, although that takes a long time. Riboflavin (vitamin B2) acts as a photosensitizing and photoactivating agent to speed up the process. The interaction of ultraviolet-A and riboflavin leads to crosslinking within the collagen and intracellular matrix of the stroma, thus strengthening of the cornea.
In the traditional collagen crosslinking, the surgeon first removes epithelial surface cells to facilitate penetration of the riboflavin. The next step is to administer riboflavin drops every two minutes for 30 minutes, then expose the cornea to ultraviolet-A (365 nm for 30 minutes at a power of 3 mW per cm2, for a total dose of 5.4 J). The surgeon places a bandage contact lens for five days to promote healing of the epithelial cells and improve patient comfort, and prescribes antibiotic and anti-inflammatory drops for about one week.
Decreased progression
RC, our 52-year-old patient with corneal ectasia, underwent uncomplicated CXL under a clinical trial protocol. One year later, maximum keratometry had improved to 57.40 D and best spectacle-corrected visual acuity was now 20/50-.
Like RC, other patients have shown significant improvement at one-year follow-up. For example, in a multicenter prospective clinical trial, my colleagues and I randomized 205 patients with progressive keratoconus and 175 with post-LASIK ectasia to undergo CXL or a sham treatment with riboflavin alone.3
A year later, the CXL group generally were stable and showed a decrease in corneal steepness by an average of 1.70 D while controls tended to get worse. Looking at individual eyes, we found that 31% of the patients who had CXL improved by 2.00 D or more on corneal topography vs. 3.5% who worsened.
Other studies have shown the cornea continues to stabilize and visual acuity improve two or more years following CXL.4
Post-CXL values
We also performed studies that evaluated the following values:
• Corneal topography indices. In 71 eyes (49 with keratoconus, 22 with ectasia), we found significant improvements in the index of surface variance, index of vertical asymmetry, keratoconus index and minimum radius of curvature at one year after crosslinking.
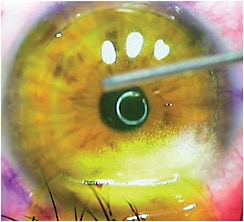
LASIK Xtra. Note the retracted LASIK flap and riboflavin solution on the treated bed.
• Higher-order aberrations. We looked at both corneal and total wavefront higher-order aberrations in 96 eyes (64 with keratoconus, 32 with ectasia) of 73 patients treated with CXL, and used a fellow-eye control group of 42 eyes. One year after crosslinking, higher-order aberrations were significantly improved compared with the control group. Mean values decreased significantly for total ocular higher-order aberrations, total coma, third-order coma, trefoil and spherical aberration.6
• Visual acuity. Uncorrected acuity showed an average improvement from 20/137 at baseline to 20/117 one year later.7Vision remained stable in most patients and substantially improved (2 Snellen lines or more) in 32%. About 12% of eyes lost 2 or more lines of uncorrected visual acuity.
Perhaps more important than uncorrected visual acuity is best spectacle-corrected vision. Patients improved, on average, about one line from 20/45 to 20/34. Most remained stable, 22% improved by 2 lines or more and about 3.5% worsened.
• Subjective vision. We gave patients pre- and postoperative questionnaires to evaluate criteria such as night driving, glare, star bursts and haloes.8 Many of these visual function symptoms got a little better after crosslinking.
• Characteristics influencing outcomes. To identify what made a patient an ideal candidate for the procedure or contraindicated crosslinking, we analyzed gender, age, cone steepness, visual acuity and corneal thickness to see which preoperative characteristics would predict a good outcome.9
Looking at corneal topography on an individual basis, we found substantial improvement in about 30% of patients and slight worsening in 3.5%. Specifically, those patients whose cones were 55.00 D or greater were 5.4 times more likely to flatten by 2.00 D or more, suggesting that patients whose keratoconus was worse were more likely to improve afterward.
Looking at BSCVA, patients generally gained about 1 line of visual acuity. About 22% improved and 3.5% lost 2 lines. Patients whose BSCVA was 20/40 or worse preoperatively were about six times more likely to improve by 2 or more lines, while those at 20/30 or better had a slightly greater risk of losing 1 line.
These results suggest that, besides stabilizing disease, CXL may benefit patients in terms of corneal topography and visual acuity. Patients at greater likelihood of such clinical improvements may be selected on the basis of how bad their vision and keratoconus are to start with.
A BETTER WAY OF HEALING?
The epi-on, epi-off debate
In each of these studies, patients actually appeared worse at one month postoperatively, with somewhat steeper cones and worse vision — a reflection of the clinical time course of CXL. Specifically, we found that patients develop haze that peaks at one month after surgery, plateaus at three months and significantly decreases between three and 12 months.10
The haze likely occurs because of keratocyte apoptosis and repopulation as well as changes in the microstructure of the collagen lamellae and glycosaminoglycans. The topography and vision changes early in the clinical time course of CXL likely are related to the healing and remodeling of the corneal epithelium.
But, would leaving the epithelium in place reduce the healing time? We are beginning to look into this, and a number of investigators are working on transepithelial techniques. The advantages to not removing the epithelium may include faster recovery, less discomfort and less potential for infection. The disadvantages: The procedure may not be as effective as epi-off CXL.
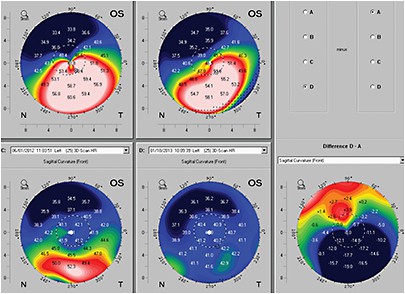
Corneal topography maps show how CXL combined with other procedures can influence corneal steepness: preoperative topography (top left); topography one year after crosslinking (top right); one month after topography-guided PRK (bottom left); one month after implantation of one 450 um Intacs segment inferiorly (bottom center); difference between preoperative and postoperative (bottom right). Note 18.00 D of maximal flattening with greatly improved corneal symmetry.
Three hurdles to clear
Three potential hurdles exist in transepithelial treatments. The first is riboflavin penetration. Riboflavin is a large, hydrophilic molecule which does not readily pass through the lipophilic epithelium. In addition, riboflavin solutions have typically contained dextran, which further prevents absorption through the epithelium.
Second, the epithelium itself as well as riboflavin in the epithelial layer will absorb UV and diminish the energy delivered to the stroma.
Finally, retaining the epithelial layer may decrease diffusion of oxygen into the stroma, impacting crosslinking pathways that depend on oxygen.
Targeting riboflavin absorption
Knowing these impediments to a transepithelial CXL approach and with the investigation of new drugs and delivery systems, we have found we can facilitate proper absorption of riboflavin for successful treatment. For example, studies have shown that benzalkonium chloride and ethylenediamine tetra-acetic acid (EDTA) can enhance epithelial permeability.11
So, we may be able to enhance that uptake by changing the make-up of the riboflavin, such as using a riboflavin solution without dextran and modifying the osmolarity of the riboflavin solution, and using adjunctive substances such as benzalkonium chloride and EDTA.11,12 Also, by using higher UV power in the accelerated crosslinking approach or longer UV exposure times, we may be able to improve the crosslinking effect of epi-on CXL.
Early results from 20 patients who underwent epi-on crosslinking show that keratometry improved by an average 0.90 D. Uncorrected visual acuity improved by almost 1 line uncorrected and by 0.5 line corrected. This is an ongoing study, and we hope to have more results later this year.
CXL AND ADJUNCTIVE APPROACHES
PRK before or after?
In the case of RC, our patient, he wanted to further improve his vision, so he had topography-guided PRK overseas. Uncorrected visual acuity improved to 20/60 uncorrected and 20/50 with +1.00 -2.75 x 50. Maximum keratometry flattened to 53.10 D.
Overseas, researchers such as A. John Kanellopoulos, MD, have focused on same-day topography-guided PRK followed by CXL vs. performing CXL followed by topography-guided PRK six months later.13
They have performed partial topography-guided PRK followed by CXL and have found it to improve visual function safely and effectively. Same day collagen crosslinking combined with topography-guided PRK has been found to be superior to sequential procedures for visual rehabilitation.14
Specifically, the crosslinking halts the progress of keratoconus, and topography-guided PRK reduces the spherocylindrical refraction and aberrations.14 Stability and progressive improvement occurs over time, although limitations may exist for steeper and thinner corneas.
For example, Dr. Kanellopoulos’ group found that 27 of 32 eyes achieved uncorrected and corrected distance visual acuity of 20/45 or better.15Twenty-seven of 32 eyes had an improvement in UDVA and CDVA of 20/45 or better (2.25 logMAR) at last follow-up. Four eyes showed some topographic improvement but no improvement in CDVA. One of the treated eyes required a subsequent penetrating keratoplasty. Two eyes exhibited grade 2 corneal haze.
CXL and Intacs
As with PRK, Intacs (OASIS Medical, Glendora Calif.) also shows promise when combined with CXL for stabilizing the cornea and improving corneal topography and symmetry.
Remember, the primary goal of Intacs is to improve corneal curvature and symmetry, allowing the patient to be fit with contact lenses more easily and to improve spectacle tolerance.16 The intrastromal corneal ring segments flatten the central corneal curvature and improve the symmetry of topography when spectacles or contact lenses otherwise are no longer effective in improving visual acuity.17
Although keratoconic eyes can tolerate the implants long term, the segments do not arrest or slow keratoconus progression; instead they address the refractive consequences of the pathology by changing the shape of the cornea, hence the need for CXL.
CXL technologies on the horizon
Several other cornea crosslinking technologies are now under study. These include:
• Accelerated crosslinking. Unlike the standard crosslinking procedure, which involves 3 mW of UVA exposure for 30 minutes, a clinical trial is evaluating a new unit, the KXL System (Avedro, Waltham, Mass.), that would allow for 30 mW and a four-minute treatment. It increases UVA power but decreases exposure time, giving the total desired dose. Powers up to 45 mW are being investigated in other studies. A trial also is under way for Pulsed Accelerated Cross‐linking. As the name suggests, this approach uses pulsed rather than continuous UVA light, with a treatment time of eight minutes. The off- phase of the light allows for more oxygen diffusion which, in turn, may enhance oxygen availability and generate more crosslinking effects.
• Topography-guided crosslinking. The KXL2 unit, introduced overseas, relies on an active eye tracker to allow a patterned delivery of UV light. Both the power and pattern can be programmed into the unit guided by the patient’s topography. In a procedure called PiXL (photorefractive intrastromal crosslinking), guided focal crosslinking is being developed for correction of refractive errors. These are for normal, non-keratoconic corneas to correct lower degrees of myopia, hyperopia and astigmatism. These are brand new applications that are beginning to be studied overseas and showing promising results.
• LASIK Xtra. In clinical studies now under way in the United States, this approach uses crosslinking as an adjunct to standard LASIK. It has two goals: to improve the strength of the cornea and avoid post-LASIK ectasia, and to reduce the regression of refractive outcomes in patients with higher degrees of myopia or hyperopia. We are participating in a multicenter clinical trial in the United States using LASIK Xtra in eyes with 2.00 D or more of hyperopia or hyperopic astigmatism. LASIK Xtra is approved outside the United States and has shown good accuracy, predictability and safety in both high myopes and high hyperopes.18
• Keraflex. This procedure, performed with the Vedera System (Avedro) uses a circle or arc of microwave energy to flatten the cornea and adjunctive crosslinking to stabilize the cornea. We are currently performing Keraflex in a clinical trial. Early results of our single-center study look promising, with marked degrees of flattening seen in some patients.
Most clinical studies have reported improvement in BCVA with a flattening of the cornea by 2.00 D to 3.00 D.16 However, the improvement in corneal symmetry can be dramatic. We have found up to 10.00 D of local flattening in some cases. Thus, it is important to define the goal of Intacs placement in a particular patient and select segment size and symmetry (and, in some cases, the use of only one segment) to optimize the outcome.
Keraflex microwave procedure one day postoperatively. Note the ring and riboflavin during crosslinking procedure.
Our patient RC still experienced persistent monocular diplopia after his topography-guided PRK, so we placed a single 450-µm Intacs segment inferiorly. Afterward, maximum keratometry decreased to 44.70 D, and BSCVA was 20/30+. Both the symmetry of corneal topography and subjective diplopia showed improvement.
My colleagues and I recently performed a physician-sponsored single-center study in which we randomized patients to receive Intacs and CXL the same day or Intacs three months after undergoing CXL. Although we are still analyzing the data, both methods have proven successful with a good safety profile. Early analysis does not show a significant difference between concurrent and sequential Intacs and crosslinking.
Conclusion
Some 30 years ago, when I first started treating keratoconus, options were limited. Crosslinking, either by itself or combined with other procedures, is the first treatment to halt the progression of keratoconus, as it did for our patient RC. OM
REFERENCES
Spoerl E, Huhle M, Seiler T. 1. Induction of cross-links in corneal tissue. Exp Eye Res. 1998;66:97-103.
Spörl E, Huhle M, Kasper M, Seiler T. Increased rigidity of the cornea caused by intrastromal crosslinking. 2. Ophthalmologe. 1997;94:902-906.
Hersh PS, Greenstein SA, Fry KL. Corneal collagen crosslinking for keratoconus and corneal ectasia: One-year 3. results. J Cataract Refract Surg. 2011;37:149-160.
Agrawal V. Long-term results of cornea collagen crosslinking with riboflavin for keratoconus. Indian J Ophthalmol. 4. 2013;61:433-434.
Greenstein SA, Fry KL, Hersh PS. Corneal topography indices after corneal collagen crosslinking for keratoconus and corneal ectasia: one-year results. J Cataract Refract Surg. 5. 2011;37:1282-1290.
Greenstein SA, Fry KL, Hersh MJ, 6.berrations after corneal collagen crosslinking for Hersh PS. Higher-order a keratoconus and corneal ectasia. J Cataract Refract Surg. 2012;38:292-302.
Hersh PS, Greenstein SA, Fry KL. Corneal collagen crosslinking for keratoconus and corneal ectasia: One-year 7. results. J Cataract Refract Surg. 2011;37:149-160.
Brooks NO, Greenstein S, Fry K, Hersh PS. Patient subjective visual function after corneal collagen crosslinking for keratoconus and corneal ectasia. J Cataract Refract Surg. 8. 2012;38:615-619.
Greenstein SA, Hersh PS. Characteristics influencing outcomes of corneal collagen crosslinking for keratoconus and ectasia: implications for patient selection. J Cataract Refract 9. Surg. 2013;39:1133-1140.
Greenstein SA, Fry KL, Bhatt J, Hersh PS. Natural history of corneal haze after collagen crosslinking for keratoconus and corneal ectasia: Scheimpflug and biomicroscopic analysis. J 10. Cataract Refract Surg. 2010;36:2105-2114.
Spadea L, Mencucci R. Transepithelial corneal collagen crosslinking in ultrathin keratoconic corneas. 11. Clin Ophthalmol. 2012;6:1785-1792.
12. Raiskup F, Pinelli R, Spoerl E. Riboflavin osmolar modification for transepithelial corneal cross-linking. Current eye research. 2012;37:234–238.
Kanellopoulos AJ. Comparison of sequential vs same-day simultaneous collagen crosslinking and topography-guided 13. PRK for treatment of keratoconus. J Refract Surg. 2009;25:S812-818.
Krueger RR, Kanellopoulos AJ. Stability of simultaneous topography-guided photorefractive keratectomy and riboflavin/UVA crosslinking for progressive keratoconus: case reports. J 14. Refract Surg. 2010;26:S827-832.
Kanellopoulos AJ, Binder PS. Management of corneal ectasia after LASIK with combined, same-day, topography-guided partial transepithelial PRK and collagen crosslinking: the 15. Athens protocol. J Refract Surg. 2011;27:323-331.
Vazirani J, Basu S. Keratoconus: 16. current perspectives. Clin Ophthalmol. 2013;7:2019-2030.
Hovakimyan M, Guthoff RF, Stachs O. Collagen crosslinking: current status and future directions. J Ophthalmol. 17. 2012;Epub 2012 Jan 12.
Celik HU, Alagöz N, Yildirim Y, et al. Accelerated corneal crosslinking concurrent with laser in situ 18. keratomileusis. J Cataract Refract Surg. 2012;38:1424-1431.
| About the Author | |
| Peter Hersh, MD, is founder of The Cornea and Laser Eye Institute-Hersh Vision Group, Teaneck, N.J. He is a professor and director of the Cornea and Refractive Surgery Division at Rutgers Medical School, visiting research collaborator at Princeton University and team ophthalmologist for the New York Jets of the National Football League. Disclosure: Dr. Hersh disclosed he is a medical monitor for Avedro. |
|